CBBLE UDHC SIMILAR CASES
CASE OF A- DKA SECONDARY TO ? FOURNIER'S GANGRENE.
15 February 22
THIS IS AN ONLINE E LOG BOOK TO DISCUSS OUR PATIENT'S DE - IDENTIFIED HEALTH DATA SHARED AFTER TAKING HIS / HER /GUARDIAN'S SIGNED INFORMED CONSENT .HERE WE DISCUSS OUR INDIVIDUAL PATIENT'S PROBLEMS THROUGH SERIES OF INPUTS FROM AVAILABLE GLOBAL ONLINE COMMUNITY OF EXPERTS WITH AN AIM TO SOLVE THOSE CLINICAL PROBLEMS WITH COLLECTIVE CURRENT BEST EVIDENCE BASED INPUT
A 60 year old male ,teacher by occupation, was brought to casualty in a drowsy state since yesterday, fever since 2 days , vomitings since yesterday
HOPI:- Patient was apparently asymptomatic 30 years back then he had fever, following which he took some medication at local health centre after which patient had ? Allergic reactions and since then he is feeling that something is happening to him for which the patient consulted a psychiatrist and got treated . Since then the patient was on Tab. Fluoxetine.
H/o giddiness 25 years back for which patient went to a local hospital and got diagnosed with hypertension and was started on Tab. ATEN-AM 50/5 mg OD.
During a routine health check up 20 years back , patient was diagnosed with Diabetes mellitus and started using Tab. Glimi M1 OD
H/o gradual painless diminision of vision 10-15 years back for which the patient consulted an ophthalmologist and was diagnosed with cataract.
Patient retired 2 years back, and stopped taking DM and HTN medication as he was feeling well since then , but kept using irregularly
One month back , his daughter committed suicide and expired following which he got disturbed psychologically and started excess consumption of alcohol.
Patient now presented with h/o fever since 2 days, low grade associated with 20 episodes of vomitings since yesterday, non projectile, non bilious, with food particles as content. Not associated with pain abdomen, no SOB, associated with generalized weakness.
Past history:-
Patient is a k/c/o DM since 20 years and is in Tab. Glimi M1 OD
K/c/o HTN since 25 years and is on Tab. ATEN- AM 50/5 mg OD
GENERAL EXAMINATION:-
Patient is slightly drowsy, coherent and cooperative
Icterus present
No signs of pallor, Cyanosis, lymphadenopathy, edema
Vitals:-
Temp:- Afebrile
BP:- 100/80 mmhg
PR:- 71 bpm
RR:- 22 cpm
Spo2- :- 99% at room air.
GRBS- High.
SYSTEMIC EXAMINATION:-
CVS- S1, S2 heard, no murmurs
RS - Bilateral air entry present, NVBS heard.
Per abdomen:- Obese , non tender, scrotal abscess present ?fournire's gangrene
CNS:- NAD
Before debridement
After debridement
Surgery referral done:-
-3x2 CMS necrotic patch over scrotum
-Pus discharge present
-Induration present around scrotal abscess.
Sent for swab and pus culture and sensitivity.
? Fournier's gangrene
Investigations:-
CBP:- Hb- 10.1 g/dl
TLC- 28,000 cells/mm3
Platelets-3.64
RFT:-
Urea-101 mg/dl
Creatinine- 1.4 mg/dl
Na- 128 meq/litre
K+ - 4.7 mEq/L
Cl- 90 mEq /L
LFT:-
TB - 4.63
DB -0.17
AST -33
ALT- 16
ALP -333
TP- 6.0
Alb- 2.6
USG ABDOMEN AND PELVIS:-
Impression:- Grade 1 prostatomegaly
Bilateral renal calculi.
Serology- negative
RTPCR - Negative
PT- 18
INR -1.3
APTT - 37 secs
BT - 2 mins 30 secs
CT - 5 mins
TREATMENT:-
1) INJ. MAGNEX FORTE 1.5 gm IV/ BD
2) INJ. CLINDAMYCIN 600 mg IV TID
3) IVF NS @ 150ml/ hr
4) INJ. HAI 40 units in 39 ml NS IV @6 ml/hr >/< according to GRBS
5) INJ. NORADRENALINE 1 Amp in 49 ml NS @ 6 ml/hr >/< to maintain MAP >/= 65mmhg
6) INJ. PAN 40 MG IV OD
7) INJ. ZOFER 4 mg IV / TID
8) INJ. THIAMINE 1 amp in 100 ml NS IV OD
9) BP/ PR/ Spo2 / GRBS monitoring every hourly
10)Strict input / output charting
SOAP NOTES DAY 2

S - pain at surgical site decreased, delayed responsiveness decreased
O - pt is C/c/c
Oriented to time, place, person
Bp - 110/70 mmHg on NA @ 5ml/hr
PR 80bpm
RR 20cpm
Spo2 - 98% on RA
Grbs:- 95 mg/dl
CVS - S1 S2 HEARD, no murmurs
RS - BAE present, NVBS
P/A - soft and nontender, bowel sounds present, scrotal abcess (? Fournier gangrene) present.
CNS - NAD
Abg done at 7:45 am:-
pH - 7.51
PCO2 - 20.4
PO2 -90.8
Hco3 - 20.5
Anion gap- 16.6
Urine for ketone bodies- negative.
A - DKA with septic shock secondary to Fournier gangrene with depression
P- taper and stop insulin & NorAdrenaline infusion
Psychiatry referral.
16/2/22
FBS - 127 mg/dl
CUE- Alb : nil ; Sugars +
Hemogram- Hb - 10.4 g/dl ;TLC - 22,700
N/L/E/M :- 86/07/01/06
Plt- 3.27
LFT:-
TB 0.63
DB 0.13
AST 29
ALT 12
ALP 220
TP 5.4
Alb- 2.5
Serum creatinine 0.8 mg/dl
Serum electrolytes:/
Na - 132
Potassium - 3.1
Cl - 99
SOAP NOTES DAY 3:-
S - pain at surgical site decreased, delayed responsiveness decreased . Patient is feeling symptomatically better.
O - pt c/c/c
Oriented to time, place, person
Bp - 130/70 mmHg
PR -80bpm
RR -20cpm
Spo2 - 98% on RA
CVS - S1 S2 HEARD, no murmurs
RS - BAE present, NVBS
P/A - soft and nontender, bowel sounds present, scrotal abcess (? Fournier gangrene present)
CNS - NAD
A - DKA with septic shock secondary to Fournier gangrene
Alcohol harmful use ?psychosis under remission.
P-
1) INJ. MAGNEX FORTE 1.5 gm IV/ BD
2) INJ. CLINDAMYCIN 600 mg IV TID
3) IVF NS @ 100ml/ hr
4)INJ. PAN 40 MG IV OD
5)INJ. ZOFER SOS
6)INJ. THIAMINE 1 amp in 100 ml NS IV OD
7)BP/ PR/ Spo2 / GRBS monitoring every hourly
8)Strict input / output chart
9)INJ . KCL 2 amp in 500 ml NS over 4 hrs.
10)TAB. PREGABALIN 75 mg H/S
11)SITZ BATH TID
12) Inj. HAI 40U in 39ml NS IV @ 2ml/hr ( stopped today morning and bridged with SC insulin)
Patient on sitz bath
17/2/22
CBP:- Hb- 9.8
TLC - 13,800
Plt- 3.1
RFT :- UREA- 11
Creatinine- 0.8
Na- 137
K - 2.9
Cl- 93
LFT
TB 0.63
DB 0.17
AST 19
ALT 09
ALP 201
TP 5.1
ALB 2.39
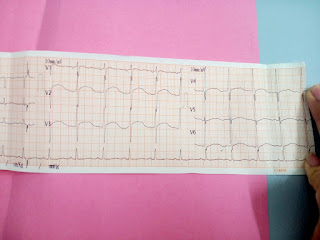
ECG
18/2/22:-Hypokalemic changes reverted back in ECG
serum K+ correction from 2.9 to 3.5
serum K+ 3.5
Blood urea - 13 mg/dl
Hb - 9.2 g/dl
Serum creatinine- 0.8 mg/dl
TLC- 9,200 cells/mm3
|
DATE
|
WBC (cells/mm3)
|
|
15/2/22
|
28,000
|
|
16/2/22
|
22,700
|
|
17/2/22
|
13,800
|
|
18/2/22
|
9,200
|
|
DATE
|
SERUM K+(mEq/l)
|
|
15/2/22
|
4.7
|
|
16/2/22
|
3.1
|
|
17/2/22
|
3.5
|
|
18/2/22
|
3.5
|
20/2/22













Comments
Post a Comment